


Beverly Anderson, Mishka Terplan, MD, and Saman Asad Siddiqui, MD, MMSc, National Center for Health Research
The concept of the IUD (Intrauterine device) as a method to prevent unplanned pregnancies has been around for a century. IUD technology has advanced significantly since they were first introduced to Americans in the 1920s, but the perception of other devices, such as the 1970’s Dalkon Shield, leaves many women with outdated views about their safety and effectiveness. More recent IUDs have an improved design that is a safer and more effective form of birth control compared to older models. They are among the most reliable forms of birth control, with pregnancy rates potentially lower than tubal ligation.1 IUDs may be a good option for women looking for a long-term, reversible form of contraception. But before deciding if this option is right for you, it is important to understand the different types of IUDs, how they work, and the risks and benefits involved.
What is an IUD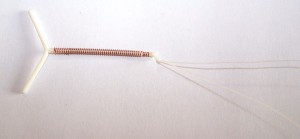
An intrauterine device (IUD) is a small, T-shaped piece of flexible plastic that is placed inside the uterus to prevent pregnancy. There are two types of IUDs available: hormonal (Mirena, Skyla, Kyleena, and Liletta) and copper (ParaGuard).2 As of 2019, the IUD is the most common form of reversible birth control in the world, used by about 159 million women.3 Although only 10.4% of reproductive-age (aged 15–49) women in the United States use long-acting reversible contraception, including IUDs, this number is quickly growing.4 In fact, it is the number one form of birth control used by gynecologists in the U.S. for their own birth control needs.5,6
How do IUDs work?
IUDs work to prevent pregnancy by several different mechanisms. It is important to understand that the IUD does not cause abortions. Rather, an IUD prevents pregnancy from occurring in the first place. Both types of IUDs physically interfere with sperm so they cannot reach the egg for fertilization.
The hormonal IUD releases a small amount of a synthetic hormone, progestogen, at a constant rate for several years. This hormone is a progestin, and it is very similar to the progesterone naturally produced by a woman’s ovaries each month. The progestogen sometimes prevents ovulation from occurring–in other words, an egg is not released from an ovary. “Additionally, the progestogen thickens a woman’s cervical mucus and causes it to become sticky, which hinders sperm movement and therefore decreases the chance of fertilization.7 If ovulation occurs and an egg is released, these changes help prevent pregnancy because 1) the thickened cervical wall blocks sperm from traveling to the site of fertilization and 2) the sticky uterine lining is a poor environment for an egg to implant and grow.
The copper IUD contains no hormones. It has a small copper wire wrapped around the plastic base of the device. Its primary method of contraception is to physically block the sperm, because copper is toxic to sperm, making it harder for them to fertilize the egg.8 This makes the IUD an extremely effective method of birth control.
Who can get an IUD? How are they inserted?
Originally, IUDs were only prescribed to women who had at least one child. The insertion process was much easier and less painful for women who have already given birth, but recent improvements in the mechanisms of insertion have made IUDs available for all women. The Mirena IUD is not recommended for women who have had breast cancer within the past five years; however, the copper IUD is still safe for these women. Additionally, patients with an active, untreated, or recently treated sexually transmitted infection (STI) should not receive an IUD. However, individuals with a history of an STI can still get an IUD.
During the insertion process, a medical professional will sometimes administer a local anesthetic to reduce the pain associated with placing the IUD. This may not be necessary for women who have given birth vaginally in the past, but guidelines suggest that all patients be advised about options to reduce the pain that can be caused by inserting the IUD, such as lidocaine that can be applied to the area.9After insertion, it is important to periodically check the strings on the IUD that hang into the vagina to make sure it is still in place. The strings are very thin and will become softer over time. You should schedule a follow-up appointment with your physician four to six weeks after the IUD is placed for them to check the strings. The strings are rarely felt during intercourse.
What are the benefits of getting an IUD?
The biggest benefit to getting an IUD is that you don’t have to worry about birth control for 3 to 10 years, depending on the type of IUD. The manufacturers of the Mirena IUD guarantee that the device lasts for up to five years, but research has suggested that it is effective for up to eight.10 The ParaGuard IUD lasts for at least ten years, and the newest IUD, Skyla, will last for three years. Additionally, IUDs are extremely effective at preventing pregnancy. Our research on tens of thousands of women found that IUD failure rates result in pregnancy for fewer than 3% of patients during the first year and is thought to be similar in subsequent years.1 Although this is not quite as effective as the 99% that is often claimed, our research shows that it is more effective than sterilization using Essure or tubal ligation (“getting your tubes tied”) and the chances of infection and pelvic pain are also lower with IUDs than with sterilization.
There are specific benefits for each type of IUD as well. The progesterone in the hormonal IUD may reduce menstrual bleeding and cramping, as well as decrease your risk of anemia. The copper IUD can be used as a method of emergency contraception if it is inserted within five days after unprotected sex. Since the copper IUD contains no hormones, there is no risk of weight gain, mood changes, or other adverse reactions to increased progesterone levels. The cost of an IUD can range from $0 (with some health insurance plans, Medicaid, etc.) to 1,300.11 This may seem like a high up-front cost, but when compared to birth control pills, which cost about $30 per month, an IUD is a cheaper method when used for more than two years. In fact, in a 2013 study that compared 15 different methods of contraception, the IUD proved to be the most cost-effective.
What are the disadvantages and risks of getting an IUD?
Neither type of IUD protects against sexually transmitted infections (STIs) or HIV. Additionally, both types of IUDs require a clinic visit for insertion and removal. Studies indicate that between 2 and 6% of the time, the IUD is rejected within the first year, and in some cases, the woman doesn’t realize her IUD is no longer in place.12 When the IUD falls out, this is called expulsion. Expulsion of the IUD can happen at any time but is less common after it has been in place for a year. Expulsion of the IUD does not cause harm, but the patient is no longer protected from an unplanned pregnancy and a healthcare provider will have to re-insert the IUD. However, if a woman has one expulsion, the chances of a second expulsion are much higher than the first time.
The copper IUDs can cause longer, heavier periods with the potential to cause anemia. In more than 10% of patients, the hormonal IUD may cause irregular bleeding for 3-6 months following insertion, though regular periods may stop completely at this point. In more than 10% of patients, it can also cause ovarian cysts.13 More than 5% of patients complain of each of the following complications: acne, headaches, pelvic pain, depressed mood, or other symptoms that are similar to those of oral contraceptives.12
A study published in 2024 of more than 150,000 women aged 15-49 years found that those using a hormonal IUD were slightly more likely to develop breast cancer than women who were not using any type of hormonal birth control.14 The researchers found that women who started using a hormonal IUD at the start of the study were 40% more likely to develop breast cancer compared to women of the same age who were not using any hormonal birth control at the time they enrolled in the study, but since most young women do not develop breast cancer, the chances for any woman with a hormonal IUD still averaged below 1%. Women who used a hormonal IUD for more than 10-15 years were more likely to develop breast cancer than those using IUDs for fewer years, but the chances were still very low. However, even that small increase could be of concern for women who are already at high risk of developing breast cancer because of family history, smoking, or other reasons.
The most serious immediate risk of any IUD is the potential for it to perforate (or puncture) the uterus at the time it is placed in a woman’s body. Although the chances of this occurring are reported to be only 1 in 1,000, it can require surgery to remove the IUD, and in rare cases, the uterus must be removed, causing infertility.
Bottom Line
Overall, the IUD is an extremely effective and safe form of birth control for most women. It is cost-effective and requires very little thought after insertion. If you’re interested in getting an IUD, talk to your physician about your options!
All NCHR articles are reviewed and approved by Dr. Diana Zuckerman and other senior staff.
- Schwarz, E.B., Lewis, C.A., Dove, M.S. et al. Comparative Effectiveness and Safety of Intrauterine Contraception and Tubal Ligation. J GEN INTERN MED 37, 4168–4175 (2022). https://doi.org/10.1007/s11606-022-07433-4
- Carey, E. (2023, May 5). Comparing IUD brands: Mirena, Skyla, Liletta, Kyleena, and Paragard. Healthline. Retrieved November 8, 2024, from https://www.healthline.com/health/birth-control/mirena-paragard-skyla#how-iu-ds-work
- United Nations. (2021). World Social Report 2021: Reconsidering rural development [PDF]. United Nations Digital Library. Retrieved November 8, 2024, from https://digitallibrary.un.org/record/3849735?v=pdf
- Centers for Disease Control and Prevention. (2020, October). Use of contraception among women aged 15-49: United States, 2017-2019 (Data Brief No. 388). National Center for Health Statistics. https://www.cdc.gov/nchs/products/databriefs/db388.htm
- Trussell, James. “Reducing Unintended Pregnancy in the United States.” Contraception Editorial January 2008. N.p., Jan. 2008. Web. June 2013.
- Stern, L. F., Simons, H. R., Kohn, J. E., Debevec, E. J., Morfesis, J. M., & Patel, A. A. (2015). Differences in contraceptive use between family planning providers and the general population: results of a cross-sectional survey. Contraception, 91(6), 464–469.
- Mayo Clinic. (2023, April 19). Mirena IUD: About this procedure. Mayo Clinic. Retrieved November 8, 2024, from https://www.mayoclinic.org/tests-procedures/mirena/about/pac-20391354
- Tamaya, T., Nakata, Y., Ohno, Y., Nioka, S., Furuta, N., & Okada, H. (1976). The mechanism of action of the copper intrauterine device. Fertility and Sterility, 27(6), 766-773. https://doi.org/10.1016/S0015-0282(16)41950-3
- Centers for Disease Control and Prevention. (2024, March 24). U.S. medical eligibility criteria for contraceptive use, 2024 (MMWR Recommendations and Reports, Vol. 73, No. RR-3). https://www.cdc.gov/mmwr/volumes/73/rr/rr7303a1.htm
- Bayer. (2022, August 17). Mirena® from Bayer approved in the U.S. for extended duration of use in contraception. Retrieved November 8, 2024, from https://www.bayer.com/media/en-us/mirena-from-bayer-approved-in-the-us-for-extended-duration-of-use-in-contraception/
- Planned Parenthood. (n.d.). How can I get an IUD? Planned Parenthood. Retrieved November 8, 2024, from https://www.plannedparenthood.org/learn/birth-control/iud/how-can-i-get-an-iud
- Healthwise Staff. “Intrauterine Device (IUD) for Birth Control.” HealthLinkBC. N.p., 2 July 2012. Web. June 2013.
- Newcomer C. for Cynthia Collins, Regulatory Review Officer, Division of Drug Marketing, Advertising, and Communication. Letter to Fadwa Almanakly, Associate Director, Advertising and Promotions, Bayer HealthCare Pharmaceuticals, December 30, 2009. http://https://www.scribd.com/document/156498192/Mirena-Warning-Letter-From-Department-of-Health-To-Bayer-Challenging-Misleading-and-Unsubstantiated-Statements
- Mørch, L. S., Meaidi, A., Corn, G., Hargreave, M., & Wessel Skovlund, C. (2024). Breast Cancer in Users of Levonorgestrel-Releasing Intrauterine Systems. JAMA, 10.1001/jama.2024.18575. Advance online publication. https://doi.org/10.1001/jama.2024.18575